近日,我院卫生管理与政策研究所团队题为“Strengthening financial protection through multi-tiered health coverage: Evidence from 667,055 low-income households in China”的研究在全球卫生政策与体系研究领域的权威期刊BMJ Global Health发表。BMJ Global Health是由英国British Medical Journal(BMJ)出版集团主办的全球卫生领域重要期刊,同时被SSCI与SCI收录,2024年JCR影响因子为6.1(五年影响因子为7.1)。根据2024年Scopus CiteScore排名,BMJ Global Health在Health Policy领域的320个期刊中位列第9,CiteScore为11.7。在2025年中科院期刊分区表(升级版)中,该期刊被列为医学大类1区、Top期刊。
文章简介:
我国实行的“基本医保+大病保险+医疗救助”多层次医疗保障体系为解决全球性“因病致贫”难题提供了中国方案。我院卫生管理与政策研究所团队基于陕西省66.7万户低收入家庭医疗救助大数据的研究证实,多层次医疗保障体系显著降低了低收入就医家庭的灾难性卫生支出发生率(从58.59%降至17.89%)和因病致贫率(从41.43%降至13.47%),展现了中国医改的突出成效。
然而研究发现,该体系在改善财务困境的同时,却意外加剧了不同收入家庭间的不公平——即更贫困的家庭本就承担了更多的财务风险,且这种不公平性在医疗保障补偿后被进一步扩大。这表明医疗保障资金的分配机制仍需优化。值得期待的是,信息技术和人工智能的发展为实施更精准、更合理的医疗保障补偿提供了新机遇。
本研究具有以下意义:一是通过大样本数据证实了我国多层次医疗保障体系对于低收入家庭财务保护的关键作用;二是揭示了医疗保障体系对财务保护公平性的影响机制;三是为全球卫生治理提供了“广覆盖+多层保障”的中国方案,特别是为中低收入国家实现全民健康覆盖目标贡献了中国智慧。
文章作者:Guanping Liu, Zhongliang Zhou, Yangling Ren, Xiaohui Zhai, Yan Zhuang, Zhichao Wang, Ruifeng Cui
文章链接:http://doi.org/10.1136/bmjgh-2025-019440
文章部分图形展示:
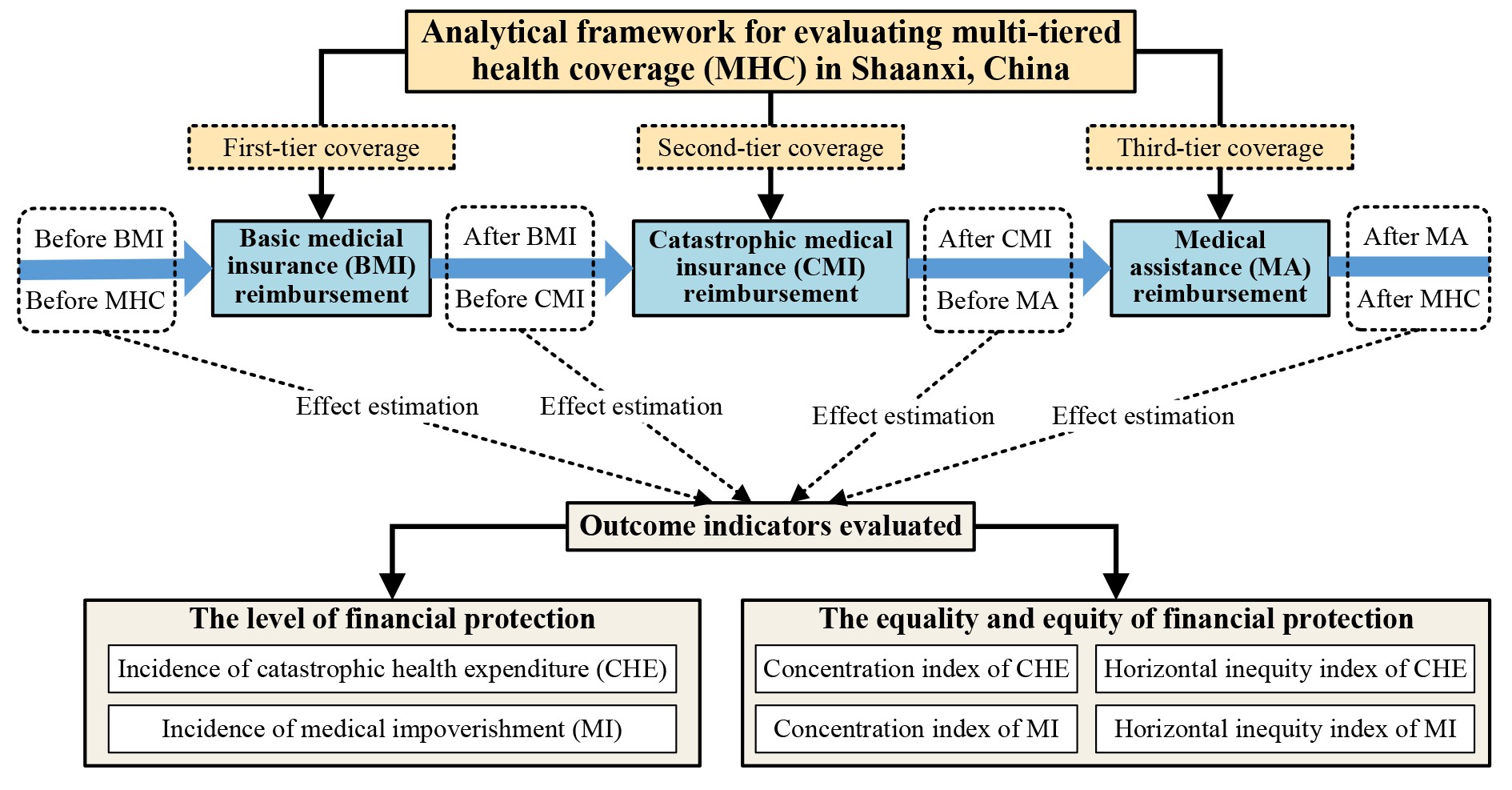
Appendix figure A2. Analytical framework for evaluating multi-tiered health coverage (MHC) in Shaanxi, China. MHC: multi-tiered health coverage; BMI: Basic Medical Insurance; CMI: Catastrophic Medical Insurance; MA: Medical Assistance; CHE: catastrophic health expenditure; MI: medical impoverishment.
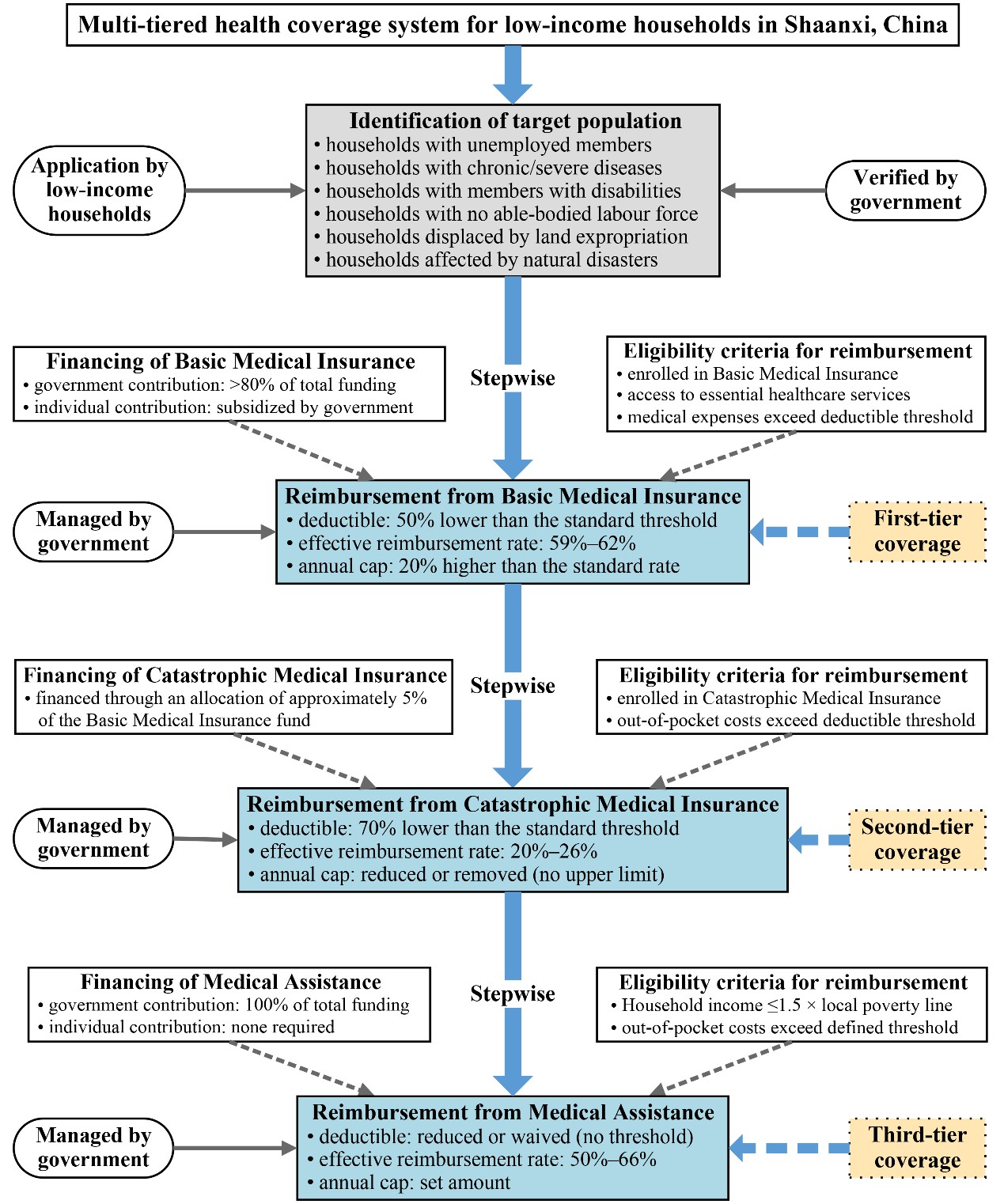
Figure 1. Structure and operational features of the multi-tiered health coverage system for low-income households in Shaanxi Province, China. The diagram illustrates the institutional framework and operational flow of China’s multi-tiered health coverage system for low-income households, comprising basic medical insurance (BMI), catastrophic medical insurance (CMI), and medical assistance (MA). Coverage proceeds in a stepwise manner, with each tier activated upon meeting defined eligibility criteria and reimbursement thresholds. Each scheme operates under its own set of rules—including deductibles, reimbursement rates, and annual caps. Shaded blue boxes represent the components evaluated in this study, based on administrative data from 2013 to 2016. Effective reimbursement rates reflect the actual reimbursement received as a percentage of total medical expenses, rather than the nominal policy rates.
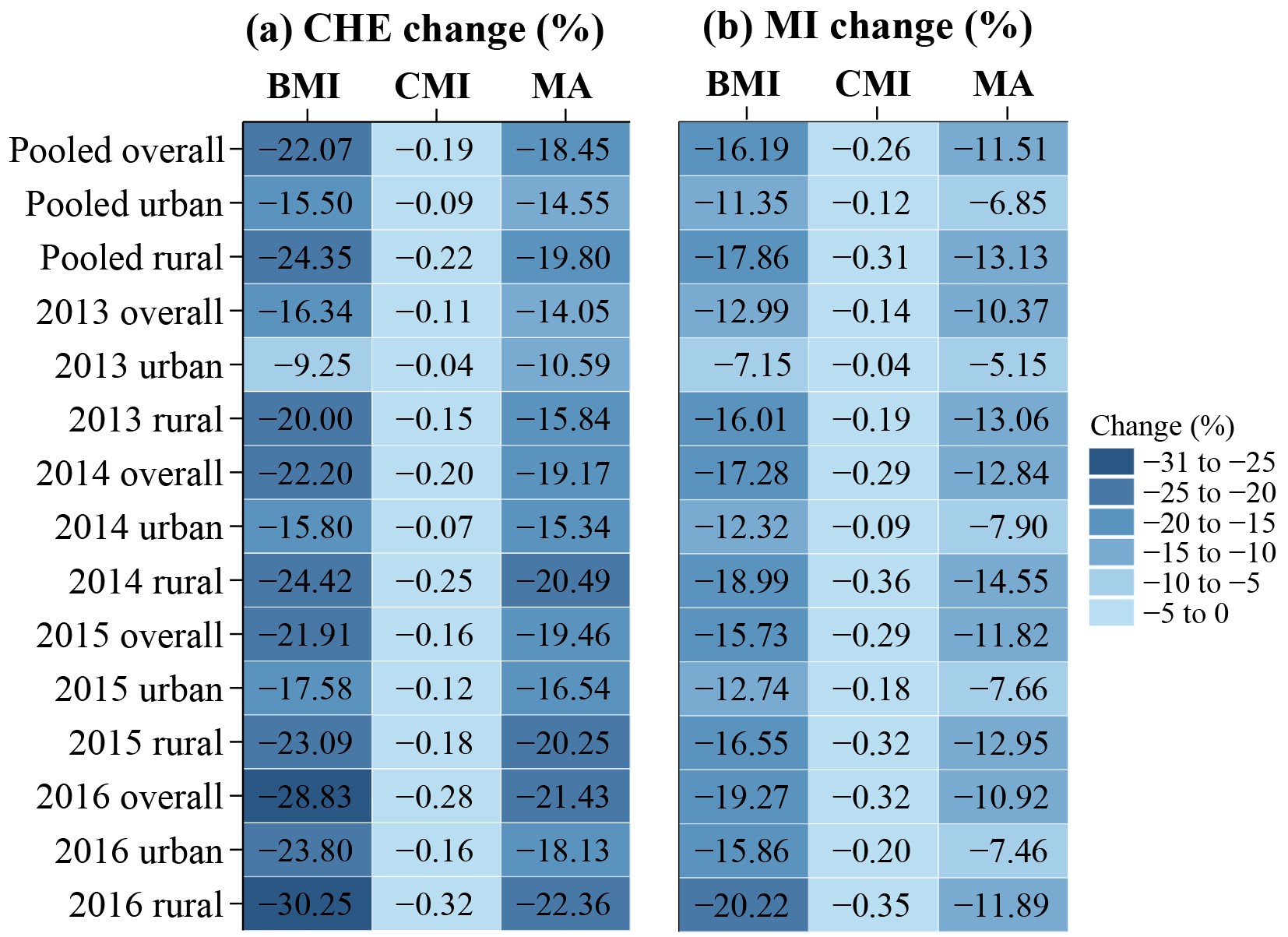
Figure 2. Percentage-point changes in CHE incidence after reimbursement through China’s multi-tiered health coverage system. Heatmaps display changes in the incidence of (a) catastrophic health expenditure (CHE; 25% threshold) and (b) medical impoverishment (MI; USD 1.90 threshold), after reimbursements from basic medical insurance (BMI), catastrophic medical insurance (CMI), and medical assistance (MA). Results are shown for pooled and annual subgroups stratified by urban–rural status. All changes are negative. Darker shades indicate larger reductions in incidence. Full numerical results are reported in supplemental appendix table A5.
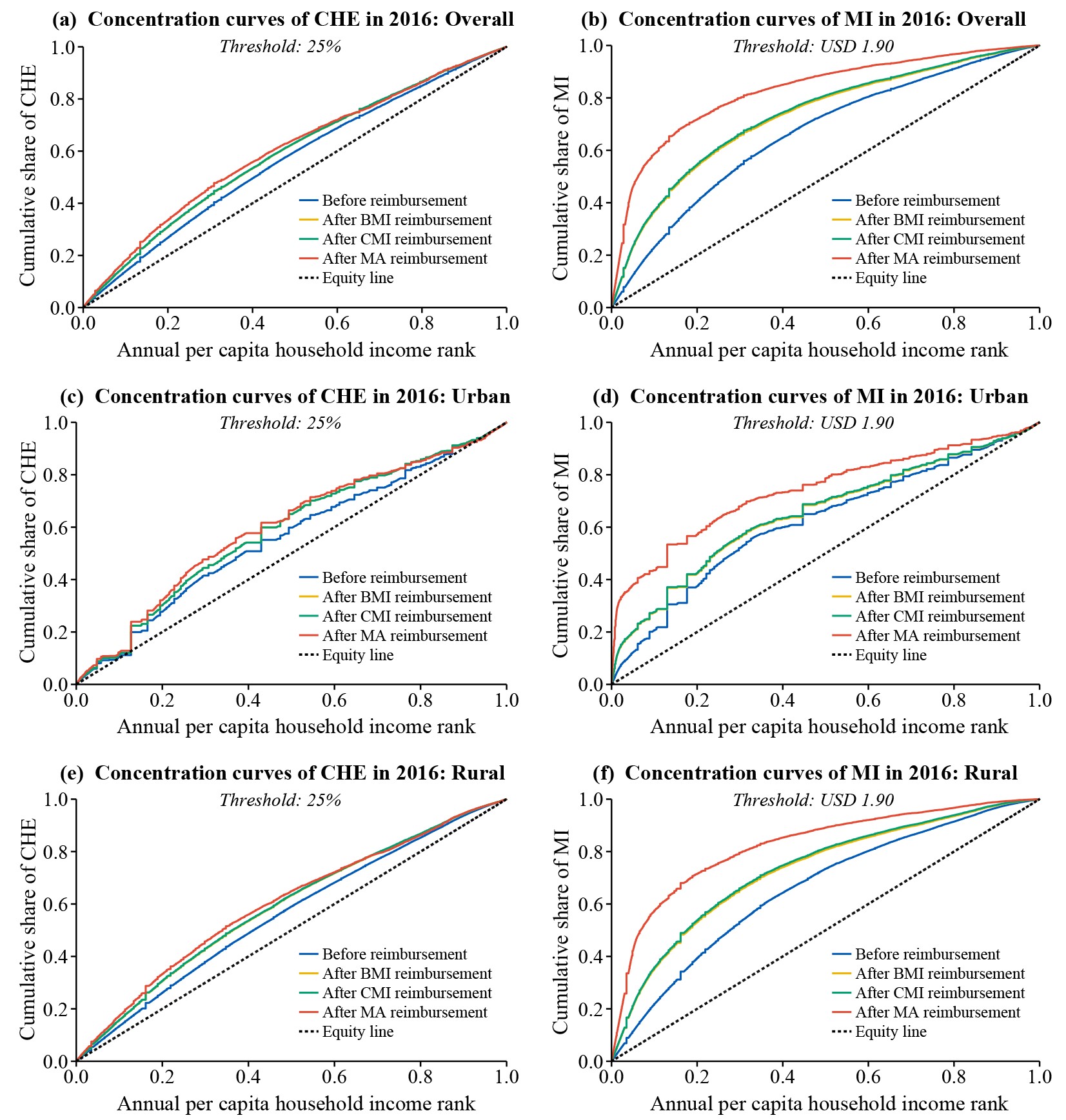
Appendix figure A7. Concentration curves of catastrophic health expenditure (CHE) and medical impoverishment (MI) in 2016: overall and by urban–rural residence.
